by Carl V Phillips
I recently had the opportunity to give a talk at what was basically the wake for the end of the quarter-century run of the wonderful Robert Wood Johnson Foundation Scholars in Health Policy Research program at the University of Michigan. I chose to put together some themes from my work as a tribute to one of the goals of that program, bringing the thinking of serious social scientists into health policy arenas where it is desperately lacking. Alas, most of my fellow alumni focus on engineering a better medical system or medical financing, with few choosing to try to deal with public health (let alone “public health”). Medical practice is obviously extremely important, but not so desperately in need of imported thinkers. Well, at least you have me.
I got some great feedback on this talk making that alone well worth my effort. (Thanks to all my colleagues. And it was great seeing you. We’ll be in touch.) But I wanted to also share what I created more broadly here. The following are my slides from the talk, with some text to explain what is not fully contained in the slides, along with a bit of extra material that was not in the talk.

Live versions of those links, for those who do not recall those essays: first, second. See also the two follow-up posts to the first of those.

You may recall a few months ago the kerfuffle that was created when CDC told all women who were capable of getting pregnant that they should not let a drop of alcohol pass their lips, and instructed medics to badger them about this. Not only was this a far more stringent recommendation than is supported by the science, but it clearly demonstrated the lack of recognition of any human preference other than maximizing health outcomes.
This generated a lot of bad press, but really only because it was politically incorrect. If the target of this aggressive shaming and disregard for humanity had been men — let alone tobacco product users — it probably would have passed without a peep of pushback from the chatter press. As it usually does…

While the bullying is concentrated in the “public health” faction, the failure to recognize real human preferences is present throughout public health. Consider the Zika recommendations:
“So how long should we delay pregnancy? Is there an end to this in sight? Should we go out and contract Zika now so that we can get pregnant later, after we are mostly immune to a new acute infection?”
“We have no idea. We’ll get back to you. Just delay pregnancy until you hear from us. What’s the big deal?”

That last bit is critical, so it is worth emphasizing. It unethical to use government and quasi-governmental force in pursuit of a special-interest goal that is not shared by most people. It is insane to assume that everyone shares that goal and base your “science” on that assumption.
For those not familiar, the latter point is a true story. Public health types genuinely insisted that people would not change their behavior as a result of HIV treatment improvements, and expressed shock when the inevitable change occurred. And these were not the “public health” people whose rhetoric might be explained by pure special-interest posturing. The innumeracy is not limited to them. These are the same infectious disease people, or their mentors from the previous generation, who are now suggesting delaying pregnancy in the face of Zika because technological change will (we hope) lower the risk soon, at which point the behavior can be more safely resumed. The mind boggles at the contradictions. The analogy to lowering the health costs of tobacco use is nearly perfect.

Readers of this blog will recall the previous post, about the direct harm inflicted by “denormalizing” campaigns and other efforts to punish smokers and other tobacco product users. Though I did not address the point there, the blithe acceptance of such abusive policies can be seen as an outgrowth of this same innumeracy. Recall also my analysis, in the “Why is there anti-THR?” series, of how the dream of a tobacco-free world is a major motivator for anti-THR efforts. While the goal is motivated by a special-interest political preferences, the innumerate failure to recognize that it is an absurd fantasy is critical for perpetuating the dishonesty, wasted resources, and massive loss of welfare that result from that goal.
I have discussed extensively on this page how the FDA’s “MRTP” rules, if taken at face value, mean that no product or claim can ever be approved. Simple economics tells us that of course there is going to be someone out there in our huge population who is right below the margin for choosing to use tobacco products, but will consume a new lower-risk product or an existing product upon learning it is low risk. Thus, even setting aside the fact that both a time machine and unimaginably precise research methods would be needed to support the mandated claim, simple economics tells us the condition will never be met. I have speculated that this might be tactics rather than innumeracy on the part of its architects: FDA’s decisions about tobacco products have all been arbitrary rather than process-driven, and this condition lets them refuse any application they want to refuse. But even if this is true, the fact that they can get away with such a patent absurdity is still a product of the pervasive innumeracy.
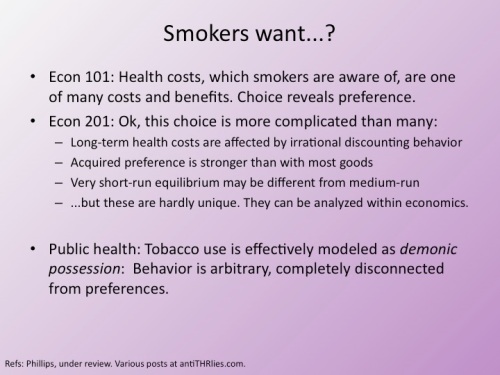
For those who may not know, the first point refers to the economic principle of “revealed preference”, in which we (for good reason) believe that the best evidence of preferences can be found in actual choices. Talk is cheap. Public health research methods that ostensibly translate cheap talk into assessments of preferences are utter jokes.
I have developed the “demonic possession” concept over time on this page and elsewhere. For those wanting a specific reference, see here.
Live link to our paper that explores the second-order preferences concepts and some of the other points in the slide.
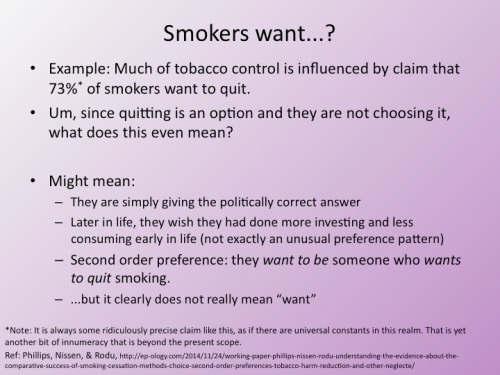
To expand in the concept in the footnote: There is nothing in epidemiology that is not specific to a particular population and time. Any reference to an epidemiology results needs to be presented in the context of those variables, and any suggestion that a result is a constant across people and time is ludicrous, as Burstyn and I noted in this lesson. Any assessment of behavior or preference is even more subject to change across time and space, as well as based on exactly how the question is posed. Yet public health authors make claims as if one survey result is a universal constant (including when, as in this case, it is clearly not an accurate measure). This is not economic innumeracy specifically, but rather an innumeracy within public health of even its own core sciences.
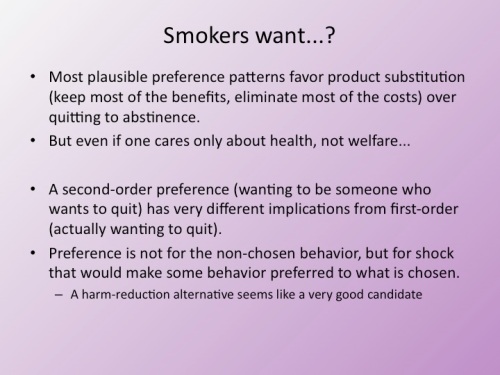
The first point there is quite important, and I perhaps should have given it a full slide. Undoubtedly some smokers have a preference pattern such that smoking is their preferred choice (as demonstrated by their actual choice) and abstinence is next-best, beating out even their most preferred low-risk alternative. It might simply be they really dislike all of the alternatives, or it might be there is a dynamic such that while they prefer to continue to smoke, if the continuity of their behavior were broken they would be happiest not consuming any product. But for most preference patterns, whatever someone’s tradeoff among health, the consumption benefits, and other factors, if smoking (with its great health costs) is preferred to abstinence, abstinence will be inferior to one or more low-risk alternatives, since their health costs are indistinguishable from abstinence, but they keep some of the smoker’s benefits from smoking.
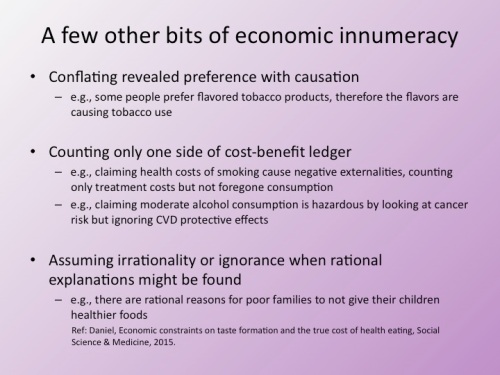
The first example is common, though it may not be obvious it is a case of economic innumeracy; just because flavor X is demonstrably preferred to flavor Y, it obviously does not mean that abstinence is preferred to flavor Y (which is implicit in the claim that flavor X is causing consumption). The second example is one of the dominant myths of tobacco control, and is frequently repeated by vaping advocates. Smoking clearly saves the rest of society resources (money) despite the rationalization for punitive taxes that it is costly. For medical care alone it is so close to a wash that it is impossible to distinguish from the null (dying from a smoking-caused disease means not consuming any subsequent medical care), but if you add in other foregone consumption the health impacts clearly create a net cost savings. The third example will be familiar to those who follow the UK’s nanny state follies, because this is currently being touted by government officials and their sock puppets as a reason for avoiding moderate drinking.
The fourth example requires some explanation if you have not read the paper or the popular press coverage. This is one of my favorite recent examples. The typical attitude from public health types is that poor people are just too stupid to make good decisions for themselves. So when they feed their children less-than-healthy food, it is obviously due to their ignorance or irrationality. After all, insist the public health types, a healthy diet is just as affordable as an unhealthy one, and so the plebes just need some convincing at the hands of Whole Foods shoppers. Enter Ms. Daniel, who actually did some research on real human motivations and discovered that people facing genuine food insecurity — who are desperately worried about what little food they can afford going to waste — do not dare try something new and different. They know intuitively what research also shows, that getting a kid to try a new food typically takes a half-dozen tries, during which a lot of food is wasted. All parents know that, but most of us do not give the waste a second thought. Some people do not have that luxury, so they stick with the chicken nuggets that they know will be eaten.
There has been a decades-long running joke about tensions between the economists and sociologists in the RWJF Scholars program. I noted in the talk, only half jokingly, that when a sociology student (Ms. Daniel) can point out that you are being economically innumerate — as with public health assuming utter irrationality for a repeated and very important decision, rather than seeking a rational explanation for the behavior — you know you are really doing something wrong. (See also: demonic possession and tobacco use.)
Yes, the talk was given on April 1, giving me a perfect opportunity to make this point, which I have made here dozens of times (the slide was animated so only the title appeared at first). “Public health” people consistently write whatever political conclusion they personally support and attach it to every research paper, even if it is no way supported by (or even flatly contradicted by) the study results. But even apart from that, all manner of public health people almost always tack on a call for some half-assed policy intervention to every research report. This demonstrates a very deep economic innumeracy, failing to recognize that every action has costs that must be identified weighed against the benefits. Moreover, many proposed actions will not even produce the benefits (i.e., solve the problem the research purportedly demonstrates) that they kinda sorta sound like they will produce. Recall my policy analysis (or the shorter blog post covering some of the points) of the FDA e-cigarette deeming regulation, which showed the policy will probably not further any of its own stated goals, and will clearly be counterproductive for many of them.
Of course “teach public health people some economics” is an intervention, though obviously not one that I just thoughtlessly concocted. It has no apparent downsides when measured in terms of bettering the world. I both thank and curse the Scholars program, and my mentors and colleagues from it, for helping me become the one trying to do that.

“It has no apparent downsides when measured in terms of bettering the world.”
Now, just wait a minute there! My world is better by virtue of the fact that I regularly get to ROTFL at “public health,” thanks to your insightful blogs.
Don’t worry — you have to evaluate in terms of actual projected impact, not some perfect attainment of the theoretical optimum (like public health people do). There is no chance I will make enough of a dent to foreclose that benefit. (And, thanks :-)
Curious how this was received in-person.
Quite well by everyone I talked to, ranging up into the range of “that was great; you need to turn it into a book” (sigh). During Q&A the sort-of-pushback was mostly a matter of adding information and analysis points that I had in my pocket but that I just did not have a chance to cover, thereby leaving gaps. I got a bit stronger pushback from a group that was closest to the issue (smoking and such) but that was mostly technical and simply beyond my ability to cover in that forum; I doubt they were ultimately too hostile since they are best known (by me, anyway) for the apostate observation that lost consumer surplus needs to be considered as a negative from anti-smoking success.
Excellent post as always Carl. As I was reading it I was applying the basic economic principles you spoke of to the juggernaut that is the Tobacco21 movement. Nevermind their fallacious arguments in support of it: There is popular support for the law (like policies enacted on this basis have never come back to haunt us); we’ve noticed that people usually begin tobacco use early in life so preventing it will cause people to lose interest in it forever, etc. In economic terms, no proponent of this movement has ever acknowledged even a hint that there might be potential costs in enacting the law. The most obvious one is that by including e-cigarettes they’re significantly raising the costs for 18-20 year-olds to obtain them and thus deriving them of the benefits of using a low risk alternative that will incur health costs, not to mention the loss of welfare enhancement for that same age group who chooses to smoke. Perversely, by banning the sale of both cigarettes and e-cigarettes they are going to make the overall costs cheaper for tobacco cigarettes and increase their use. We know that using (or switching to) e-cigarettes often involves a lot of trial and error. All things being equal, why attempt to do so in the much harder to navigate grey market when a pack of smokes will still be just about as easy to obtain and work straight out of the pack? It almost as if they think banning people’s preferences will eliminate them. They seem to have no clue that their intervention will merely alter the preferences because they’re altering the costs. In this case, they think the increase costs will cause a widespread preference for abstinence. This will happen for some people, but not nearly as many as they think. Certainly not enough to make up for the overall negative effects of the policy.
Interestingly, one of my old friends at this meeting played a role in what was (or was supposed to be) an attempt to seriously scientifically evaluate the tobacco-21 stuff. The assessment was: It would not actually have any noticeable impact on 18-20 smoking rates, but it would actually put downward pressure on under-18 rates (most 18-year-olds know a 21-y-o who can buy for them; fewer 16-y-olds, who all know an 18-y-o, do). But the cost of doing that, in terms of infantilizing adults and creating horrible precedent was just enormous. I mentioned in another comment here that some others at this meeting (that I did not know personally — they were after my time) have argued for the consumer surplus point. Also (my observation), the organized black market for underage cigarette sales is pretty minimal right now, but this could make it viable and that drives down prices. After all, ten or twenty percent of kids (officially — probably actually higher, as per another discussion at this meeting) are smoking weed, and they can’t legally buy that.
It is probably true that any delay in adopting a behavior during that age range will diminish the chances it will eventually be adopted. Of course, it won’t stop it. Tobacco Controllers (e.g., US FDA) still lie that most initiation is by underage kids, but actually the median age of smoking initiation is 18 or perhaps 19. Delaying uptake did not end it. On the bright side, someone initiating tobacco use at 19 or 21 is probably much more likely to realize that smokeless or ecigs are a better option than smoking — as noted, much of the benefit and far less cost.
The real insanity of it is that an 18-year-old can make much more momentous (and thus potentially harmful) decisions than to take up smoking (going into enormous debt; joining the military). These people are so caught up in their pseudo-ethic that they probably don’t even understand this. At least with alcohol-21 there is a legitimate argument about negative externalities (and a potentially legitimate argument about developing brains, which is still almost-always-junk brain science, but it is rather more convincing than the absurd similar claims about nicotine).
I was trying just now to imagine what “public health” people think “health” actually is. One can only assume it’s something along the lines of “having your heart beat for the absolute maximum number of seconds, irrespective of every single other consideration.”
See the essay linked in the text (this one: https://antithrlies.com/2014/09/21/dear-public-health-the-public-despises-you-so-you-are-probably-doing-it-wrong/ )
Thank you for prompting me to re-read this; it’s some of your best stuff, and I ran into a number of things I’ve paraphrased in subsequent conversations without realizing it or meaning to.
There was another aspect of “public health” orthodoxy that was on my mind today (and, as with most others, it’s probably something about which you’ve already written and which I’ve already consumed). Namely, the extent to which unintended consequences never seem to enter into “public health” thinking. The thing they’re doing, or the action they propose, has only one of two potential outcomes:
1) It will have exactly the intended effect; or
2) If it appears to have any other effect, it is only due to insufficient funding and/or the machinations of some shadowy (and, obviously, evil) corporate cabal that gleefully preys on innocent children.
So I guess my question is this: do “public health” types, even amongst themselves, ever acknowledge and discuss the unintended consequences (which are numerous and, more often than not, bad) of their various ideological/political policy pursuits?
That is a good way to put it, and while I have written about the point, of course, I don’t think I ever did that one-two. So you get credit for laying it out like that. I often discuss point 1, which is a huge problem, and allude to point 2, but you put it more precisely. I do think that is right, that when their predictions about the effect of an intervention are proven wrong (which is about 99% of the time an intervention is actually tried) they manage to find a way to avoid learning from it, such as that.
The really crazy thing is that this is not just limited to cheap-talk academic papers. Recall my policy analysis of the deeming regulation (linked from the post) that shows that the rule would set back rather than further its own stated goals. FDA are about to do a real and massive policy intervention, but are already destined to go down your one-two script like they are just some random academic proposing some silly little intervention.
Pingback: Six bad arguments against criticism of misleading pro-THR claims | Anti-THR Lies and related topics